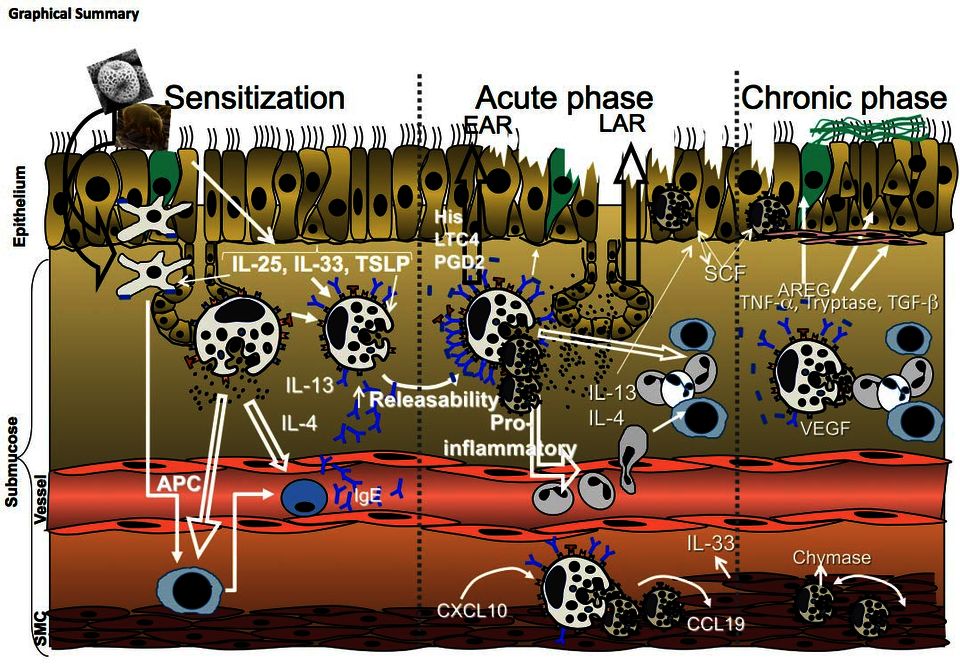
Asthma is a chronic inflammatory disease characterized by airway hyperresponsiveness, airway inflammation, and airway remodeling. Mast cells (MC) activated through IgE, and specific allergens, release mediators that drive early phase reactions (EPR), contribute to late phase reaction (LPR), and also take part in airway remodeling.
Classically MC have been seen as effector cells of the early and late asthmatic reactions. After exposure to aeroallergens they release preformed (histamine, TNF-α, proteases), and de novo synthesized mediators (e.g. LTC4, PGD2) that contribute to bronchoconstriction, oedema and mucus production featuring EAR. Cytokines (e.g. IL-4, IL-5, IL-13) mediate the LAR characterized by a submucosal inflammatory infiltrate where eosinophils and lymphocytes predominate.
In chronic asthma MC are continuously activated by FcεRI crosslinking, but also through non-IgE dependent mechanisms such as proteases, cytokines, TLR ligands, etc. In the healthy human lung, 90% of MC are of the MCT subtype, but in asthmatic patients although total mast cell count does not change, the number of MCTC is increased and localized in 3 specific sites1:
- Airway epithelium: Tryptasehigh, CPA3high, chymaselow (IEMC)2
- Airway mucous glands: Tryptase-chymase3
- Airway smooth muscle (SMC): Typtase-chymase4
MC and airway epithelium
Airway epithelial cells are among the first responders to allergens, and once stimulated they are key cells for lung dendritic cells (DC) activation to establish allergen-specific sensitization. Epithelial cells secrete innate cytokines like IL25, TSLP and IL33. These cyotkines are known to promote Th2 immunity through DC, but they also activate mast cells and basophils, an early source of IL45.
In chronic asthma, MC migrate to the epithelial cells layer. They are probably recruited by means of the effect of CCR3, CxCL8 or other chemokines. Intraepithelial MC (IEMC) can then initiate and perpetuate the Th2 response in the lungs1.
MC and AHR
Hyperresponsiveness (AHR), an exaggerated ASM reaction to nonspecific stimuli, is a cardinal feature of asthma. Persistent AHR is not fully linked to sustained inflammation, since it has been shown that corticosteroid treatment diminishes inflammation independently of airway reactivity.
MC-derived histamine, PGD2 and LTC4 are potent bronchoconstrictors. The number of MC infiltrating ASM is correlated to AHR and to asthma severity. MC infiltrating smooth muscle cells do express IL4 and IL13, two key cytokines in the development of AHR. TNF-α is also overexpressed, and has also been shown to be a potent inductor of AHR. Tryptase ability to induce bronchoconstriction and AHR in animal models suggests a likely relevance of this protease to the respiratory distress7.
MC and remodeling
MC-derived mediators have been identified as important inductors of airway remodeling1, i.e. structural changes of the lower airway:
- Subeptihelial fibrosis: amphiregulin, bFGF and tryptase are mitogenic for fibroblasts and induce collagen synthesis
- Extracellular matrix deposition can be induced by amphiregulin, plasminogen activator inhibitor-1 (PAI-1)
- Vascular remodeling: MCTC number is associated with increased vascular area and VEGF expression in asthmatic airway. Pro-angiogenic mediators produced by MC are VEGF and bFGF, but also histamine, tryptase, heparin and IL-8.
- Goblet cells metaplasia and mucus hypersecretion can be induced by amphiregulin, IL4, IL13, IL9, chymase, PGD2
- Increased ASM mass: tryptase, LTD4, activin A and PDGF can induce asthmatic ASM proliferation in ex vivo settings
Summary
MC do not only participate in EAR and LAR, but they also might be pivotal to the pathophysiology of chronic asthma. MC most probably take part in the initiation, development and propagation of the multiple asthma features. Current therapies target individual molecules13 (many of them against specific mast cell mediators, see Figure 2), however there is a need for new anti-asthmatic therapy with a broader spectrum, such as therapy targeting the release of mast cell mediators related to the pathophysiology of astma.
More about mast cells and asthma
Animal models have been useful for studying MC in disease. Among others, some of the relevant findings are;
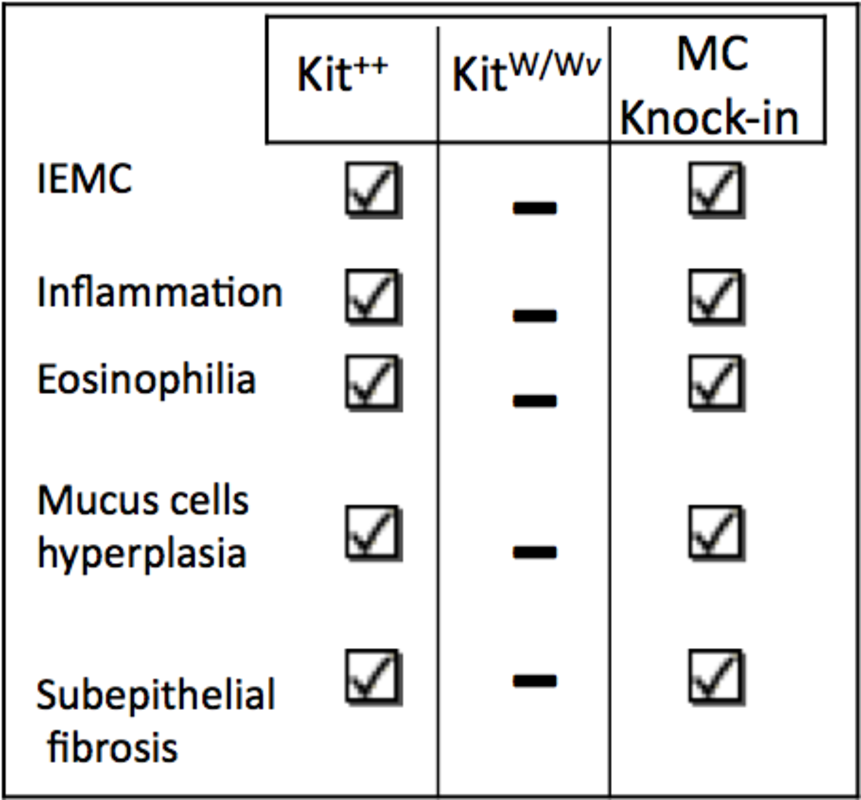
- In a rodent model of asthma MC are required to fully develop the multiple features of chronic asthma6 (Figure 1 and Table 1).
- Recruitment of mast cells to the airway is best studied in BALBc mice than in C57BL/68 but the first experiments with mast-cell deficient BALBc mice have arisen unexpected results9. New studies with novel mast-cell deficient mice strains are required10,11.
- As for our data, MC activity (upregulation of lung mMCP-1) is increased in HDM aeroallergens-induced airway pathology in mice, and it is decreased when the airways are exposed to PGE2 receptor agonists. Such decrease correlates with changes in airway reactivity and inflammation12.
References:
| 1. | Carter R &Bradding P. Curr Pharm Des; 2011,17:685-698 |
| 2. | Dougherty R et al, JACI; 2010, 125:1046-1053 |
| 3. | Carroll N et al, Thorax ;2002,57:677-682 |
| 4. | Bradding P et al, JACI ;2006, 117:1277-1284 |
| 5. | Lambrecht B & Hammad H Nat Med; 2012,8:684-692 |
| 6. | Yu M et al; JCI,2006;116:1633-1641 |
| 7. | Okayama Y et al; Curr Opin Immunol 2007,19:687-693 |
| 8. | Pae S et al, Immunogenetics; 2010, 62:499-506 |
| 9. | Becker M et al, J Immunol; 2011, 186:7225-7231 |
| 10. | Dudeck J et al, Immunity; 2011, 34:973-984 |
| 11. | Feyerabend a et al, Immunity; 2011, 35: 832-844 |
| 12. | Herrerias A Int Arch Allergy Immunol; 2009, 149:323-332 |
| 13. | Holgate S, JACI; 2011,128:495-505 |
| 14. | Galli S & Tsai M, Nat Med; 2012, 18:693-704 |


{kind=link}
{kind=link}
{kind=link}