Hallmarks of cancer
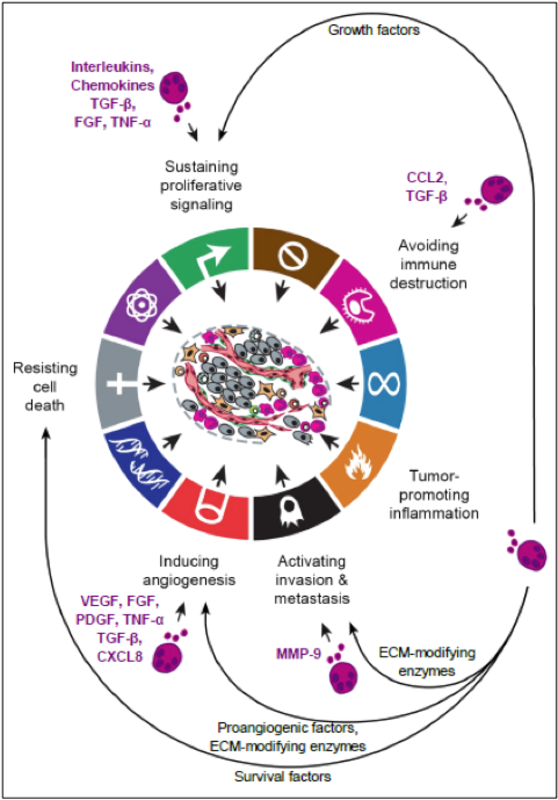
The hallmarks of cancer include, according to Hanahan and Weinberg1, ten different mechanisms, as shown in Figure 1. Inflammation plays an important role in different stages of tumor development, including initiation, promotion, malignant conversion, invasion and metastasis.2 Here, tumor-infiltrating immune cells interact with cancer cells in an extensive and dynamic crosstalk.2 Among those immune cells, mast cells have been found to infiltrate the stroma of many tumors. Although investigations on the precise roles of mast cells in tumors are still at the very beginning, mast cells have been demonstrated to actively participate in several hallmarks of cancer, as shown in Figure 1. Mast cell-derived mediators can either exert pro-tumorigenic functions, causing progression and spread of the tumor, or anti-tumorigenic functions, limiting tumor growth. Table 1 and 2 summarize mast cell mediators and their possible effects on tumor biology.
{kind=link}
{kind=link}
{kind=link}
Mast cells in tumors – Pro- or anti-tumorigenic functions?
A pro-tumorigenic role of mast cells was first suggested by Westphal in 1891, reporting on increased numbers of mast cells in tumors. Today, it is well known that various types of hematologic malignancies and solid cancers are associated with increased mast cells.3-11 In many tumors, mast cell counts have been reported to even correlate with tumor stage, prognosis and invasiveness.4-9,12 A correlation between numbers of mast cells and poor prognosis was for example demonstrated in human lymphoid neoplasms such as Hodgkin´s lymphoma7, B-cell non-Hodgkin’s lymphoma9, primary cutaneous lymphoma12 and multiple myeloma13. Similar data were obtained in human solid cancers, such as pancreatic cancer14, hepatocarcinoma8, cholangiocarcinoma8, prostate cancer4 and melanoma6,15. In a recent study on human and murine prostate tumors, mast cells were shown in detail to increase in number upon disease progression.4 Moreover, experiments using mast cell-deficient mice demonstrated that mast cells were necessary for development of transplanted well differentiated prostate tumors.4
Table 1: PRO-TUMORIGENIC
| Mediators | Effects and function |
|---|---|
| Histamine | Increase of vascular permeability, angiogenesis, immunosuppression |
| Heparin | Increase of vascular permeability, angiogenesis, matrix reorganization |
| Tryptase | Tissue remodeling, neovascularization, facilitate metastases |
| Chymase | Facilitate metastases, tissue damage and remodeling |
| NGF, SCF | Promote tumor growth, mast cell chemoattractant |
| PDGF, CSF | Promote tumor growth |
| VEGF | Angiogenesis, mitogenesis of endothelial cells |
| FGF | Promote tumor growth, neovascularization, matrix reorganization and degradation |
| TGF-β | Promote tumor growth, mitogenesis of endothelial cells, angiogenesis |
| CCL2, CCL5 | Chemoattractants for mast cells and other immune cells |
| CXCL8 | Neovascularization, matrix reorganization and degradation |
| TNF-α | Immunosuppression, neovascularization |
| IL-3, 4 | Matrix reorganization and degradation |
| Ang-1 | Angiogenesis, formation of blood vessels |
Table 2: ANTI-TUMORIGENIC
| Mediator | Effects and function |
|---|---|
| IL-1, 6, 9, 10 | Inflammation, leukocyte migration |
| IL-3 | Mast cell proliferation, eosinophil activation |
| IL-4 | Tumor cell apoptosis, TH2 differentaition |
| IL-5 | Leukocyte migration, eosinophil activation |
| TNF-α | Inflammation, tumor cell death |
| IFN-ϒ | Inflammation, leukocyte proliferation and activation |
| GM-CSF | Inflammatory cell proliferation, eosinophil activation |
| TGF-β | Inflammatory cell proliferation |
| PAF | Platelet activation, leukocyte chemotaxis |
| PGD2, PGE2 | Vasodilation, neutrophil chemotaxis |
| LTB4, LTC4 | Leukocyte chemotaxis, increase vascular permeability |
| MIP-α | Chemoattractant for monocytes, macrophages and neutrophils |
| MCP-3/4 | Chemoattractant for leukocytes |
| Tryptase | Inflammation |
| NO | Vasodilation |
The relationship between mast cell numbers and tumor invasiveness was recently evaluated in thyroid cancer.5 In this study, mast cell-derived mediators promoted in vitro proliferation, survival and invasive ability of thyroid carcinoma cells and, vice versa, human thyroid carcinoma cells induced activation of mast cells.5 In line with these observations, circulating mast cells were recruited in mouse xenografts of human thyroid cancer cells and mast cells were able to enhance xenograft growth.5 Similar results were obtained in pancreatic cancer confirming the essential role of mast cells for invasion of tumors.14 Patients with pancreatic cancer showed elevated serum tryptase levels suggesting increased numbers of mast cells and mast cell-conditioned medium induced migration, proliferation and invasion of pancreatic cancer cell lines.14 On the other hand, pancreatic cancer cells stimulated migration of mast cells.14 In murine pancreatic cancer, mast cell numbers were increased and correlated again with tumor grade and reduced survival.14 In addition to thyroid carcinoma and pancreatic cancer, supernatants of mast cells were shown to induce cytokine release and proliferation of primary cutaneous lymphoma cells in vitro.12 Similarly, mast cell infiltration was associated with a worse relapse-free survival in patients with Hodgkin’s lymphoma.7
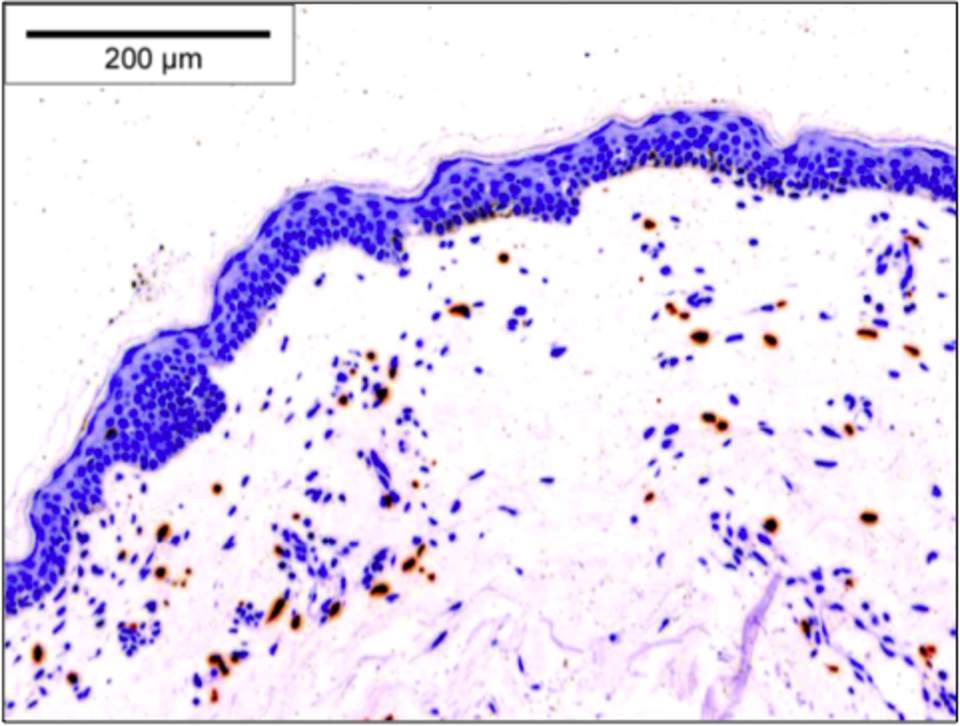
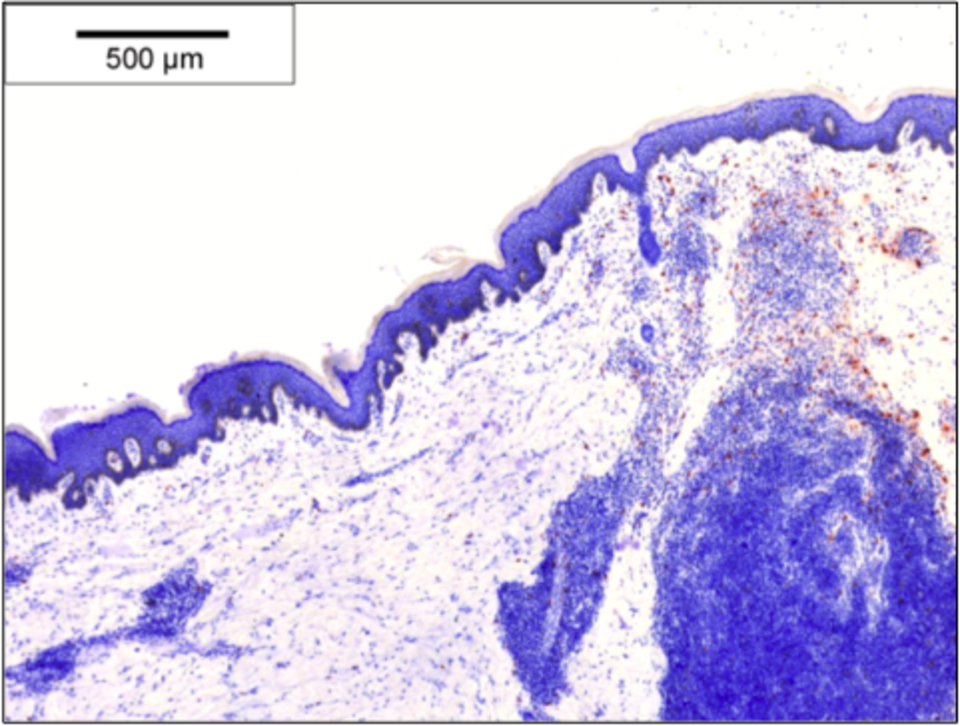
Several recent studies also suggested indirect effects of mast cells on tumors through interaction with other immune cells and blood vessels. For example in Hodgkin´s lymphoma, aggregation of eosinophils together with mast cells was described to correlate with poor prognosis.16 In various tumors including melanoma6, lung cancer17 and squamous cell carcinomas of the esophagus18 and cervix19, mast cell infiltrates correlated with microvessel density in addition to tumor progression. For example in melanoma, immunhistological stainings showed increased microvessel density correlating with mast cell numbers in lesions of poor prognosis compared to those of intermediate and good prognosis.6 Similar results were obtained for primary cutaneous lymphoma, where increased mast cell numbers (Figure 2 and 3) together with increased degranulation correlated with microvessel density and progression.12 Moreover, several studies using different tumor models observed reduced tumor neo-angiogenesis associated with decreased tumor growth in mast cell-deficient mice.12,20,21
Again supporting the concept of a pro-tumorigenic contribution of mast cells to tumors, several studies reported on decreased tumor growth upon inhibition of mast cells. For example, Gounaris et al (2007)20 showed in a murine colon cancer model that polyps are infiltrated with mast cells and depletion of mast cells either pharmacologically or through generation of mast cell-deficient chimeric mice lead to profound remission of polyps.20 Also, in a genetic tumor model for pancreatic islet tumors, in which activation of Myc triggers tumor expansion associated with recruitment of mast cells, pharmacologic inhibition of mast cell degranulation was found to inhibit tumor growth.21
On the other hand, mast cells were also shown to exert anti-tumorigenic effects in certain malignancies, for example by supporting cancer rejection.10,22 One of these studies investigated colorectal cancer, in which infiltrates of mast cells were associated with lower rates of lymph node and distant metastases.22 Furthermore, patients with low mast cell counts showed more pronounced invasion than those with higher numbers of mast cells and, accordingly, the 5-year survival rate was worse in patients with low mast cell counts compared to those with high mast cell counts.22 Also, in breast cancer, stromal mast cells were found to correlate with low grade tumors and a favorable prognosis.10 Patients with axillary lymph node metastases showed more mast cells in the non-involved axillary lymph nodes, indicating a protective effect of mast cells in breast cancer.10
In summary, a series of recent studies demonstrated specific effects of mast cells on tumor biology. In a large number of tumors, mast cell infiltrates correlate with tumor progression. However, other tumors show the opposite with an inverse correlation of mast cells and tumor growth. Moreover, infiltrates of mast cells are often associated with tumor invasion and increased microvessel density. In some tumors, mast cell counts also correlate with accumulation of other immune cells, such as eosinophils, suggesting indirect effects of mast cells. Finally, inhibition of mast cell numbers and degranulation decreased tumor growth in several experimental models. Together, these studies suggest to further explore mast cells as possible diagnostic and therapeutic target of tumors.
References:
| 1. | Hanahan D, Weinberg RA (2011) Cell 144, 646-674. |
| 2. | Crivennikov SI, Greten FR, Karin M (2010) Cell 140, 883-899. |
| 3. | Ribatti D, Crivellato E (2011) Adv Exp Med Biol 716, 270-288. |
| 4. | Pittoni P, Tripodo C, Piconese S, et al (2011) Cancer Res 71, 5987-5997. |
| 5. | Melillo RM, Guarino V, Avilla E, et al (2010) Oncogene 29, 6203-6215. |
| 6. | Ribatti D, Ennas MG, Vacca A, et al (2003) Eur J Clin Invest 33, 420-425. |
| 7. | Molin D, Edström A, Glimelius I, et al (2002) Br J Haematol 119, 122-124. |
| 8. | Terada T, Matsunaga Y (2000) J Hepatol 33, 961-966. |
| 9. | Ribatti D, Vacca A, Marzullo A, et al (2000) Int J Cancer 85, 171-175. |
| 10. | Amini RM, Aaltonen K, Nevanlinna H, et al (2007) BMC Cancer 7, 165. |
| 11. | Theoharides TC, Conti P (2004) Trends Immunol 25, 235-241. |
| 12. | Rabenhorst A, Schlaak M, Heukamp LC (2012) Blood 120, 2042-2054. |
| 13. | Nico B, Mangieri D, Crivellato E, Vacca A, Ribatti D (2008) Stem Cells Dev 17, 19-22. |
| 14. | Strouch MJ, Cheon EC, Salabat MR, et al (2010), Clin Cancer Res 16, 2257-2265. |
| 15. | Toth-Jakatics R, Jimi S, Takebayashi S, Kawamoto N (2000) Hum Pathol 31, 955-960. |
| 16. | Enblad G, Sundstrom C, Glimelius B (1993) Hematol Oncol 11, 187-193. |
| 17. | Tomita M, Matsuzaki Y, Onitsuka T (2000) Ann Thorac Surg 69, 1686-1690. |
| 18. | Elpek GÖ, Gelen T, Aksoy NH, et al (2001) J Clin Pathol 54, 940-944. |
| 19. | Benitez-Bribiesca L, Wong A, Utrera D, Castellanos E (2001) J Histochem Cytochem 49, 1061-1062. |
| 20. | Gounaris E, Erdman SE, Restaino C, et al (2007) Proc Natl Acad Sci USA 104, 19977-19982. |
| 21. | Soucek L, Lawlor ER, Soto D, Shchors K, Swigart LB, Evan GI (2007) Nat Med 13, 1211-1218. |
| 22. | Tan SY, Fan Y, Luo HS, Shen ZX, Guo Y, Zhao LJ (2005) World J Gastroenterol 11, 1210-1214. |
| 23. | Hanahan D, Coussens LM (2012) Cancer Cell 21, 309-322. |